
The pain came out of nowhere. One minute you were fine — the next, a sharp, cramping agony in your side that no comfortable position could ease. Or maybe it was different for you: a persistent dull ache in your lower back, burning when you urinate, or nausea that didn’t make sense.
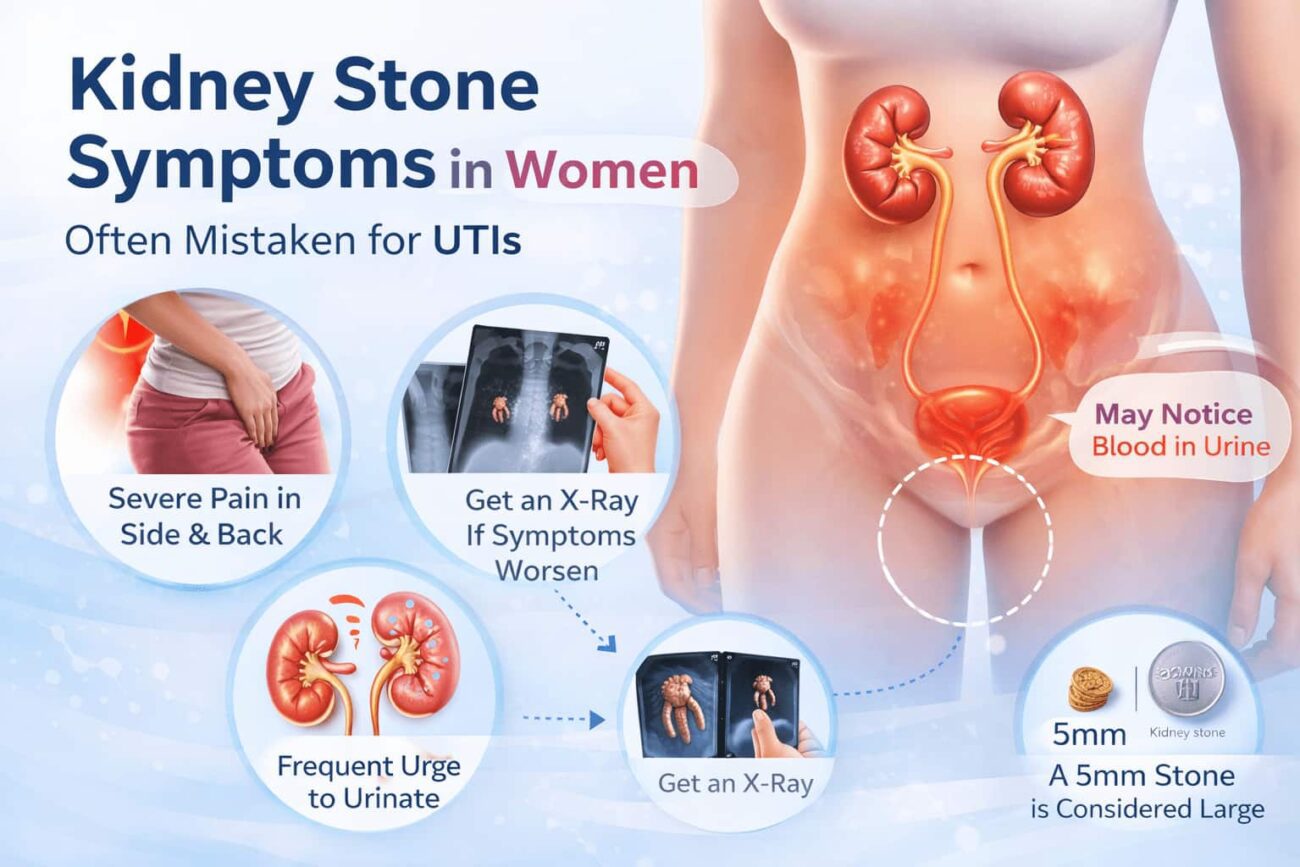
Kidney stones symptoms for women are frequently mistaken for urinary tract infections, ovarian cysts, or menstrual pain. This misidentification delays diagnosis by days or even weeks — and that matters clinically, because an untreated obstructing stone can damage kidney function.
Many women ignore early discomfort, but kidney stones symptoms for women often start as mild pain, urinary changes, or nausea before becoming severe.
This guide covers the complete symptom picture: early signs that most people miss, how symptoms differ between women and men, what a 5mm kidney stone actually means for your body, and how diagnosis — including X-ray and IVP imaging — works in practice.
What Are Kidney Stones and Why Do They Cause Such Intense Pain?
Kidney stones (nephrolithiasis) are hard mineral and salt deposits that form inside the kidneys. They develop when urine becomes too concentrated — allowing minerals like calcium, oxalate, uric acid, and struvite to crystallise and clump together.
Most stones start small and produce no symptoms at all while they remain in the kidney. The pain begins — often explosively — when a stone moves into the ureter, the narrow tube connecting the kidney to the bladder.
The ureter is only 3–4mm wide at its narrowest points. Even a 3mm stone can cause significant obstruction, triggering intense peristaltic contractions (the ureter rhythmically squeezing to push the stone through) and a dramatic spike in pressure above the blockage.
That pressure is what generates the characteristic pain: sudden, severe, cramping, typically in waves — often called renal colic. Unlike a muscle strain, it does not change with position. Lying down, sitting, or pacing all feel equally bad.
kidney stones symptoms for women Most People Miss
Early kidney stones symptoms for women include mild flank pain or a dull ache below the ribs on one side, slight discomfort when urinating, urine that appears cloudy or slightly pink, and unexplained nausea. These early signs appear before the stone moves into the ureter and often go unrecognised because the pain is not yet severe.
Recognizing kidney stones symptoms for women early can help prevent severe pain and complications, especially when symptoms are mistaken for common urinary issues.
Most people associate kidney stones with dramatic, collapse-to-the-floor pain. But that level of pain represents a stone actively obstructing the ureter — not the earlier, more manageable phase. Early kidney stone symptoms are subtle enough to be dismissed entirely.
What early symptoms actually feel like
Flank Discomfort
A persistent dull ache or pressure below the rib cage on one side, often mistaken for a pulled muscle or back strain. May come and go over days.
Pink or Cloudy Urine
Microscopic haematuria (blood in urine) occurs even before pain becomes severe. Urine may look pink, red, or smoky. This is a key early red flag.
Nausea Without Cause
The kidney and gut share nerve pathways (the celiac plexus). Even a stone sitting quietly in the kidney can trigger nausea through referred nerve signals.
Mild Urinary Burning
As a stone approaches the bladder, mild burning or urgency can begin. This is frequently and dangerously misidentified as a UTI in women.
Low-Grade Fever
Not always present, but a low fever can indicate inflammation or early infection around the stone. A high fever (above 38.5°C) with stone pain is a medical emergency.
Groin or Inner Thigh Pain
As the stone descends, referred pain travels down the ureter’s nerve distribution — into the groin, inner thigh, and genitals. Often misread as a sports injury or hip problem.
Kidney Stones Symptoms for Women vs Men: Key Differences

The core symptoms of kidney stones — renal colic, haematuria, nausea — are biologically identical in both sexes. The differences lie in how symptoms present, where referred pain is felt, and crucially, how they are interpreted by both the patient and clinician.
Recognizing kidney stones symptoms for women early can help prevent severe pain and complications, especially when symptoms are mistaken for common urinary issues.
Key differences between kidney stone symptoms in women and men:
- Women’s stone pain is more often confused with UTIs, ovarian cysts, or endometriosis — delaying correct diagnosis
- Women feel referred pain more commonly in the lower abdomen and pelvis, mimicking gynaecological conditions
- Men feel referred pain more commonly in the testicles and tip of the penis as the stone approaches the ureterovesical junction
- Women are more likely to have struvite (infection) stones, which grow larger before causing symptoms
- Men have a slightly higher lifetime risk (11% vs 9%) but women are increasingly affected — the gap has narrowed significantly since 1980
- Pregnant women face increased stone risk due to urinary stasis and calcium metabolism changes, with fewer safe imaging options
👩 Kidney Stone Symptoms: Women
- Lower abdominal or pelvic pain (often misread as period pain)
- Burning urination frequently attributed to UTI
- Nausea and vomiting alongside back pain
- Urinary urgency and frequency without infection
- Referred pain to inner thigh or vulva
- May have concurrent UTI masking stone symptoms
- Struvite stones: fewer acute symptoms, larger at diagnosis
👨 Kidney Stone Symptoms: Men
- Severe flank pain radiating to groin (classic presentation)
- Sharp pain at the tip of the penis as stone nears bladder
- Testicular or scrotal pain — often the dominant complaint
- Blood in urine usually more visible (lower baseline UTI frequency)
- Sudden-onset pain with no preceding symptoms in many cases
- Uric acid stones more common — associated with gout, high meat diets
Why women are so often misdiagnosed
A 2021 analysis of emergency department presentations found that women with kidney stones waited significantly longer for pain management than men with the same pain scores. One documented reason: their symptoms — pelvic pain, burning urination, nausea — overlap almost entirely with UTI and gynaecological presentations.
Clinically, the distinguishing factor is pain character. Kidney stone pain (renal colic) is visceral, colicky, comes in waves, and does not change with movement. Musculoskeletal pain improves with position. Ovarian pain is usually less acute and more constant. If in doubt, a urine dipstick showing haematuria without significant bacteriuria strongly points toward a stone.
What a 5mm Kidney Stone Means — And What to Expect
Stone size is the single most important predictor of whether a stone will pass on its own or require intervention. The 5mm threshold is where clinical management decisions often shift.
1–4mm — High spontaneous passage rate (80–95%)
Most pass within 1–4 weeks with adequate hydration. Conservative management (fluids, pain control, alpha-blocker medication like tamsulosin to relax the ureter) is standard.
5mm — Borderline passage rate (40–60%)
A kidney stones 5mm stone sits at the clinical crossroads. It may pass naturally over 2–6 weeks, but the chances drop significantly compared to smaller stones. Alpha-blockers increase passage rates. Active monitoring is typically required — with intervention if the stone fails to pass after 4–6 weeks or causes persistent obstruction or infection.
6–9mm — Low spontaneous passage rate (20–40%)
Medical expulsive therapy alone is often insufficient. Shockwave lithotripsy (SWL) or ureteroscopy is frequently recommended before the 4-week mark.
10mm+ — Surgical intervention usually required
Stones larger than 10mm rarely pass without intervention. Percutaneous nephrolithotomy (PCNL) is standard for stones 10mm and above or when other methods fail.
The 5mm dimension referenced in searches about “kidney stones 5mm pictures” refers to the stone’s longest measured diameter on imaging — typically CT scan or ultrasound. On an X-ray, only calcium-containing stones are visible; uric acid stones are radiolucent (invisible to X-ray) and require CT or ultrasound for detection.
Kidney Stone Diagnosis: X-Ray, CT, Ultrasound — Which Is Used and When
When a clinician suspects a kidney stone, the choice of imaging depends on availability, cost, radiation exposure, and clinical urgency.
| Imaging Type | What It Shows | Limitations | Best Used For |
|---|---|---|---|
| CT Scan (non-contrast) | All stone types, exact size, location, degree of obstruction | Radiation exposure; cost | First-line imaging in most emergency settings; most accurate |
| Kidney Stone X-Ray (KUB) | Calcium and struvite stones only (radio-opaque) | Misses uric acid and cystine stones; less precise sizing | Monitoring known calcium stones; post-treatment follow-up |
| Ultrasound | Kidney swelling (hydronephrosis), stones 5mm+ | Poor at visualising ureteral stones; operator-dependent | Pregnant women; children; initial triage; avoiding radiation |
| Intravenous Pyelogram (IVP) | Urinary tract anatomy, obstruction level | Requires contrast dye; replaced by CT in most settings | Planning surgical intervention; assessing drainage post-procedure |
Doctors often rely on imaging tests when kidney stones symptoms for women are unclear or overlap with other conditions like UTIs.
About the kidney stones diagnosis code
For those researching administrative or insurance aspects: the primary ICD-10-CM diagnosis code for kidney stones (nephrolithiasis) is N20.0 (calculus of kidney), N20.1 (calculus of ureter), and N20.2 (calculus of kidney with calculus of ureter). Renal colic without identified stone is coded as N23. These codes are used for billing, insurance claims, and medical record classification — not for clinical decision-making.
When Kidney Stone Symptoms Become a Medical Emergency
Most kidney stones, while excruciatingly painful, are not dangerous if the urinary tract remains uninfected and kidney function is preserved. However, certain combinations of symptoms require immediate emergency care — not a next-day GP appointment.
- Fever above 38.5°C (101.3°F) combined with flank pain — this suggests an infected, obstructed kidney (urosepsis risk)
- Uncontrollable vomiting preventing oral hydration
- Complete inability to urinate despite strong urges
- Pain so severe it cannot be controlled with over-the-counter medications
- Any of the above in a person with a single functioning kidney
- Stone symptoms in a pregnant woman (requires immediate obstetric and urological evaluation)
An infected obstructed kidney — pyonephrosis — is a surgical emergency. Bacteria trapped behind the stone multiply rapidly in stagnant urine, and systemic infection (urosepsis) can develop within hours. This is the one scenario where kidney stone pain becomes genuinely life-threatening.
Practical Steps to Reduce Kidney Stone Risk
Kidney stones have a recurrence rate of approximately 50% within 5–10 years without preventive measures. These evidence-based steps are the most effective:
- 1Drink 2.5–3 litres of water daily. Adequate hydration is the single most effective preventive measure for all stone types. Urine should appear pale yellow. Dark yellow urine is a consistent sign of insufficient fluid intake.
- 2Reduce dietary sodium — not calcium. High salt intake increases urinary calcium excretion, promoting stone formation. The common belief that people prone to calcium stones should restrict dietary calcium is clinically outdated — low calcium intake actually increases oxalate absorption and stone risk.
- 3Limit high-oxalate foods if you form calcium oxalate stones. Spinach, beetroot, nuts, tea, and chocolate are high in oxalate. Pairing them with calcium-rich foods (dairy, fortified plant milk) during the same meal binds oxalate in the gut, preventing urinary excretion.
- 4Moderate animal protein intake. High meat consumption lowers urine pH and increases uric acid, promoting uric acid stone formation. This is the primary dietary driver of stones in men with gout-associated nephrolithiasis.
- 5Add citrate to your diet. Citrate — found naturally in lemon juice, lime juice, and orange juice — inhibits calcium crystal aggregation in the urine. Squeezing half a lemon into water daily has measurable preventive effects, comparable in some studies to potassium citrate supplementation.
- 6Get a 24-hour urine collection after your first stone. This test measures the exact chemical composition of your urine, allowing a nephrologist to identify your specific stone risk profile and tailor prevention — rather than applying generic advice.
For detailed guidance on magnesium’s role in kidney health — including how magnesium citrate supplementation reduces urinary oxalate — see our evidence-based guide to magnesium supplementation. Magnesium competes with calcium for oxalate binding, and magnesium deficiency is consistently associated with elevated stone recurrence risk.
For official clinical guidelines, the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) provides comprehensive patient guidance on kidney stone prevention and treatment. The American Urological Association’s Medical Management Guidelines offers the clinical framework used by urologists in practice.
Frequently Asked Questions
The earliest signs are often subtle: a dull ache or pressure below the ribs on one side, mild burning when urinating, urine that looks slightly pink or cloudy, and unexplained nausea. These symptoms frequently precede the severe renal colic pain by hours or days. Because burning urination is so often attributed to UTIs in women, the stone diagnosis is frequently delayed.
The core symptoms are identical, but referred pain location differs. Women tend to feel stone pain in the lower abdomen and pelvis — mimicking ovarian or menstrual pain. Men typically feel referred pain in the testicles and groin. Women are also more prone to struvite stones (infection-related), which grow silently before causing symptoms. Misdiagnosis is more common in women.
Yes, but not reliably. A 5mm stone has approximately a 40–60% chance of passing spontaneously within 4–6 weeks. Alpha-blocker medications (such as tamsulosin) improve this rate by relaxing ureteral smooth muscle. If the stone has not passed within 4–6 weeks, causes persistent obstruction, or becomes infected, urological intervention (ureteroscopy or shockwave lithotripsy) is typically recommended.
Only certain kidney stones are visible on plain X-ray (KUB — kidneys, ureters, bladder). Calcium oxalate and calcium phosphate stones appear radio-opaque and show up on X-ray. Uric acid stones — which account for 8–10% of all stones and are more common in men with gout — are radiolucent and invisible to X-ray. Non-contrast CT scan is the gold standard for detecting all stone types with highest accuracy.
The primary ICD-10-CM codes are: N20.0 (calculus of kidney), N20.1 (calculus of ureter), N20.2 (calculus of both kidney and ureter), and N23 (unspecified renal colic). These are used for insurance billing, hospital records, and statistical reporting — not for clinical decision-making.
Active renal colic — the wave-like cramping pain of a stone in the ureter — typically lasts minutes to hours per episode and can recur over days or weeks until the stone passes. Once the stone enters the bladder, most pain resolves within hours. Passage from bladder to outside typically causes brief discomfort but rarely the severe pain of ureteral transit.
Historically, kidney stones were far more common in men (roughly 3:1 ratio). That gap has narrowed substantially — current estimates put lifetime risk at 11% for men and 9% for women. The rise in stone prevalence among women is linked to increasing rates of obesity, type 2 diabetes, and metabolic syndrome — all of which are independent stone risk factors.
Summary: Recognising Kidney Stone Symptoms Faster Means Better Outcomes
Kidney stone symptoms for women are one of the most frequently misdiagnosed presentations in primary care — because burning urination, pelvic pain, and nausea are symptoms shared with far more common gynaecological and urinary conditions.
Key points to remember:
- Early kidney stone symptoms — dull flank ache, pink urine, nausea — often precede acute renal colic by hours or days
- Women feel stone pain in the lower abdomen and pelvis; men feel it in the testicles and groin — both are referred pain from the same ureter
- A 5mm kidney stone is at the clinical crossroads: it may pass with conservative management, but requires active monitoring and likely alpha-blocker therapy
- Plain X-ray (KUB) only shows calcium stones; CT scan is the gold standard for all stone types
- High fever plus flank pain is an emergency — do not wait for a GP appointment
- Drinking 2.5–3 litres of water daily is the single most effective preventive measure for all stone types
If you suspect a kidney stone, do not self-diagnose based on internet searches alone. A urine dipstick, imaging, and in some cases blood tests are needed to confirm the diagnosis, assess obstruction severity, and guide the right management plan.
Disclaimer: This article is for informational purposes only and does not constitute medical advice. Always consult a qualified healthcare professional for diagnosis and treatment of kidney stones or any medical condition.