
Ulcerative Colitis vs Ulcerative Proctitis: What’s the Real Difference — and Why It Changes Everything About Your Treatment
Your colonoscopy results come back and the gastroenterologist says two words that sound almost identical: ulcerative proctitis. You had been bracing for ulcerative colitis. Are they the same thing? Is one worse? Does your treatment change?
These are the exact questions thousands of patients search for after a new IBD diagnosis — and most of what they find online barely scratches the surface. The truth is that ulcerative colitis vs ulcerative proctitis is not simply a matter of degree. The two conditions differ in scope, symptom pattern, treatment approach, long-term risk, and quality-of-life impact in ways that matter enormously for how you manage your health.
This guide gives you the full picture — written clearly, without dumbing it down.
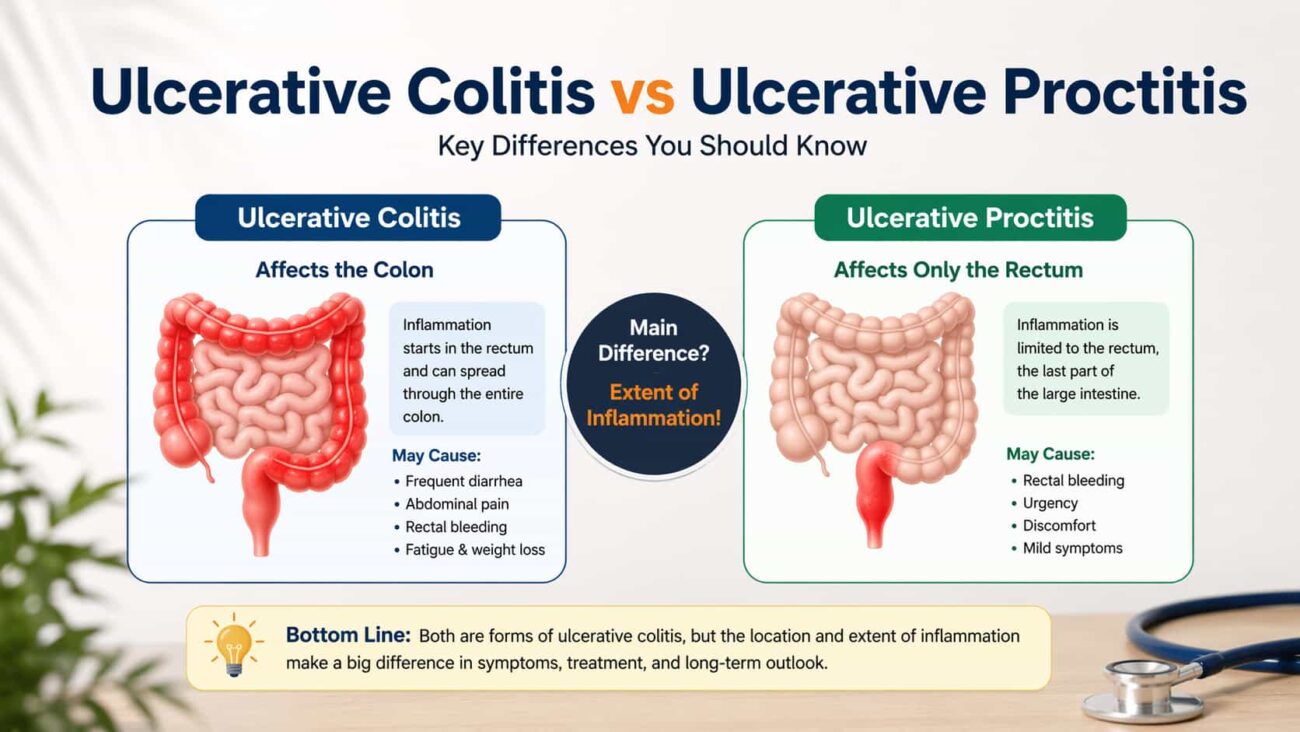
Ulcerative proctitis is a subtype of ulcerative colitis — not a separate disease. In ulcerative proctitis, inflammation is confined to the rectum only (the last 15–20 cm of the large intestine). In broader ulcerative colitis, inflammation extends beyond the rectum into the sigmoid, left colon, or the entire colon. Proctitis carries a better prognosis but requires careful monitoring for disease extension.
What Is Ulcerative Colitis?
Ulcerative colitis (UC) is a chronic, relapsing-remitting inflammatory bowel disease (IBD) that causes persistent inflammation and surface ulceration of the inner lining of the colon and rectum. It is classified as an autoimmune condition — meaning the immune system generates an abnormal inflammatory response that attacks the body’s own intestinal tissue.
UC always begins in the rectum and extends continuously upward through the colon. This continuous, uninterrupted pattern of inflammation is what distinguishes UC from Crohn’s disease, which can appear in skip lesions anywhere along the GI tract.
How UC Is Classified by Extent
Gastroenterologists use the Montreal Classification — the internationally accepted standard — to categorize UC by how far the inflammation extends:
- E1 — Ulcerative proctitis: Inflammation limited to the rectum (up to 15–20 cm from the anus).
- E2 — Left-sided colitis (distal colitis): Inflammation extending from the rectum to the splenic flexure.
- E3 — Extensive colitis (pancolitis): Inflammation beyond the splenic flexure, potentially involving the entire colon.
This classification is not just academic. It directly determines which medications are appropriate, how frequently surveillance colonoscopies are needed, and how high the long-term cancer risk is.
What Is Ulcerative Proctitis?
Ulcerative proctitis (UP) is the mildest and most localized form of ulcerative colitis. By definition, it is inflammation confined entirely to the rectum — the final segment of the large intestine before the anus.
Despite being the “mildest” classification, this label can be misleading for patients who live with it. Rectal inflammation produces intensely uncomfortable, disruptive symptoms — particularly the constant urge to pass stool and rectal bleeding — that significantly impact daily life even when the rest of the colon is completely healthy.
How Common Is It?
Ulcerative proctitis accounts for roughly 25–30% of all UC diagnoses at first presentation. It tends to be more common in older adults but can appear at any age. Despite its limited extent, it is genuinely chronic — remission can be maintained, but the disease rarely disappears permanently without treatment.
Ulcerative Colitis vs Ulcerative Proctitis: Full Comparison
| Feature | Ulcerative Proctitis (E1) | Ulcerative Colitis (E2 / E3) |
|---|---|---|
| Location of inflammation | Rectum only (≤15–20 cm) | Beyond rectum — left colon or entire colon |
| Rectal bleeding | Common — often the primary symptom | Common, often mixed with diarrhea |
| Diarrhea frequency | Mild or absent — constipation more typical | Frequent; 4–10+ episodes daily during flares |
| Tenesmus (rectal urgency) | Prominent and often severe | Present, but overshadowed by diarrhea |
| Abdominal pain | Usually mild or absent | Cramping, can be significant and widespread |
| Systemic symptoms | Rare | Fatigue, weight loss, fever, anemia |
| Extra-intestinal manifestations | Uncommon | Joints, skin, eyes, liver — up to 40% of patients |
| Colorectal cancer risk | Similar to general population | Elevated after 8–10 years; highest in pancolitis |
| Primary treatment | Topical mesalazine (suppositories) | Oral 5-ASA, immunomodulators, biologics |
| Surgery rate | Very low | Up to 20–30% over lifetime in extensive disease |
| Hospitalization risk | Low | Higher — especially during severe flares |
| Disease progression risk | 10–30% extend proximally over 10 years | N/A — already extended |
| ICD-10 code | K51.2x | K51.0x / K51.3x / K51.5x |
Symptoms Compared: What Each Actually Feels Like
The symptom profiles of ulcerative proctitis and broader ulcerative colitis overlap significantly — but the nuances matter, because they affect how quickly people recognize something is wrong and how urgently they seek care.
Symptoms of Ulcerative Proctitis
Because inflammation is restricted to the rectum, the symptom picture is localized and can be misleadingly “mild” in terms of stool frequency while being genuinely disruptive in other ways:
- Rectal bleeding: The most consistent symptom — bright red blood on toilet paper, coating stool, or in the toilet bowl.
- Tenesmus: A persistent, urgent sensation of needing to pass stool, even when the bowel is empty. This symptom can be relentless and exhausting.
- Passage of mucus: Small amounts of mucus, sometimes without stool, are common.
- Constipation: Counterintuitive but real — rectal inflammation can reduce motility in the affected segment, leading to difficulty passing stool even with urgency.
- Rectal pain or pressure: Discomfort in the lower rectum, particularly during and after bowel movements.
- Minimal abdominal cramping: Unlike broader UC, significant abdominal pain is uncommon in proctitis.
- No systemic symptoms in most cases: Fatigue, weight loss, and fever are not typical features of isolated proctitis.
Symptoms of Ulcerative Colitis (E2/E3)
- Frequent bloody diarrhea: The defining feature — during active flares, patients can pass bloody stool 6–10 or more times daily, severely disrupting sleep and daily function.
- Abdominal cramping: Often worst in the left lower quadrant before and during bowel movements.
- Rectal urgency: Present but often accompanied by actual stool passage, unlike the “false alarms” of proctitis.
- Fatigue: From chronic blood loss, inflammation, poor sleep, and nutritional depletion.
- Unintentional weight loss: Significant during active flares due to reduced appetite and malabsorption.
- Low-grade fever: Indicates active systemic inflammation.
- Anemia: Iron-deficiency anemia from chronic GI blood loss is extremely common in moderate-to-severe UC.
- Extra-intestinal manifestations: Joint pain (arthropathy), skin lesions (pyoderma gangrenosum, erythema nodosum), eye inflammation (uveitis, episcleritis), and liver disease (primary sclerosing cholangitis) occur in a significant proportion of UC patients with more extensive disease.
How Are They Diagnosed — and Distinguished?
The distinction between ulcerative proctitis and broader ulcerative colitis can only be confirmed with endoscopy. Clinical symptoms alone are not sufficient — a patient with proctitis and a patient with left-sided colitis can present with nearly identical complaints.
The Diagnostic Process
-
1Colonoscopy with biopsy The definitive test. A full colonoscopy maps the entire colon and rectum, identifying where inflammation begins, where it ends, and its severity. Biopsies taken from multiple segments confirm the histological pattern. In proctitis, the mucosa above the rectosigmoid junction appears completely normal.
-
2Fecal calprotectin A non-invasive stool test that measures intestinal inflammation. Elevated levels support an IBD diagnosis and help monitor treatment response. Useful for distinguishing IBD from irritable bowel syndrome (IBS), which produces normal calprotectin levels.
-
3Blood tests A full blood count reveals anemia. CRP (C-reactive protein) and ESR (erythrocyte sedimentation rate) reflect systemic inflammation. Serum albumin and nutritional markers flag malnutrition in more extensive disease.
-
4Flexible sigmoidoscopy Sometimes used as an initial evaluation — particularly in younger patients with rectal symptoms. It visualizes the rectum and sigmoid without requiring full bowel prep, but cannot confirm whether inflammation extends further.
-
5Ruling out infectious colitis and other causes Stool cultures, Clostridioides difficile testing, and STI screening are performed before a diagnosis of IBD is confirmed, since infections can mimic its appearance on endoscopy.
Treatment: Where Ulcerative Proctitis and UC Diverge Most
This is the section that matters most practically. The difference in treatment between ulcerative proctitis and more extensive UC is significant — both in delivery method and in the intensity of systemic medication required.
Treating Ulcerative Proctitis
The advantage of proctitis is that topical therapy — medication delivered directly to the rectum — can achieve high drug concentrations right at the site of inflammation with minimal systemic absorption.
- Topical mesalazine suppositories (first-line): Mesalazine (5-aminosalicylic acid) delivered as a suppository reaches the rectum directly. Clinical guidelines from the European Crohn’s and Colitis Organisation (ECCO) recommend this as the primary induction therapy for ulcerative proctitis. Response rates exceed 80%.
- Topical corticosteroids: Hydrocortisone or budesonide suppositories and foam enemas are used when mesalazine is insufficient or when faster symptom relief is needed. They are not suitable for long-term use due to steroid-related side effects.
- Combined oral + topical 5-ASA: When suppositories alone don’t maintain remission, adding oral mesalazine significantly improves outcomes compared to either route alone.
- Biologic agents: Reserved for refractory ulcerative proctitis that fails to respond to combined 5-ASA therapy. Though rare in proctitis, infliximab or vedolizumab may be considered in severe, treatment-resistant cases.
Treating Broader Ulcerative Colitis (E2/E3)
Treatment for left-sided colitis and pancolitis must target a larger area of the colon — making systemic therapy essential:
- Oral 5-aminosalicylates: Sulfasalazine or oral mesalazine preparations form the backbone of mild-to-moderate UC therapy. Enemas can supplement oral therapy for left-sided disease.
- Corticosteroids: Oral prednisone or IV hydrocortisone for moderate-to-severe flares. Effective for short-term induction but inappropriate for long-term maintenance due to cumulative toxicity.
- Immunomodulators: Azathioprine or 6-mercaptopurine for steroid-dependent disease — slow to act (3–6 months to full effect) but effective for maintaining remission.
- Biologic therapies: Anti-TNF agents (infliximab, adalimumab, golimumab), vedolizumab (gut-selective integrin blocker), and ustekinumab (IL-12/23 inhibitor) for moderate-to-severe or steroid-refractory UC.
- JAK inhibitors: Tofacitinib, upadacitinib, and filgotinib are newer oral targeted therapies with rapid onset — approved for moderate-to-severe UC in patients who have failed or cannot tolerate biologics.
- Proctocolectomy: Surgical removal of the colon and rectum is considered curative for UC. Indicated in medically refractory disease, high-grade dysplasia, or colorectal cancer. Most patients undergo an ileal pouch-anal anastomosis (IPAA / J-pouch) to restore continence.
Can Ulcerative Proctitis Become Ulcerative Colitis?
Yes. Ulcerative proctitis can progress to involve more of the colon over time — a process called proximal extension. Research indicates that approximately 10–30% of patients with ulcerative proctitis develop extension into the sigmoid, left colon, or beyond within 10 years of diagnosis. Extension converts the classification from E1 to E2 or E3 and typically requires a significant shift in treatment strategy.
Risk Factors for Disease Extension
Not all patients with proctitis will progress. The following factors are associated with higher risk of proximal extension:
- Inadequate or incomplete remission with initial treatment
- Persistent mucosal inflammation on follow-up endoscopy (even without symptoms)
- High fecal calprotectin levels despite clinical remission
- Extensive backwash ileitis present at diagnosis
- Primary sclerosing cholangitis as a comorbidity
- Younger age at diagnosis
- Male sex (moderately higher risk than female)
This is why treating proctitis to full mucosal healing — not just symptom relief — is the modern standard of care. Patients who achieve endoscopic remission have significantly lower rates of extension, hospitalization, and surgery.
Long-Term Risks: Cancer, Complications, and Quality of Life
Colorectal Cancer Risk
One of the most anxiety-provoking questions for any IBD patient is cancer risk. Here the distinction between proctitis and broader UC is significant:
- Ulcerative proctitis: Colorectal cancer risk is approximately the same as the general population. Surveillance colonoscopy is generally recommended after 8–10 years, but the frequency is lower than for pancolitis.
- Left-sided colitis: Moderately elevated colorectal cancer risk. Surveillance colonoscopy every 1–2 years is recommended after 8–10 years of disease.
- Pancolitis: The highest risk category — relative risk is estimated to be 5–15 times that of the general population after 20+ years of disease, particularly with ongoing inflammation. Annual surveillance colonoscopy with targeted biopsies is standard.
Quality of Life Impact
It would be a mistake to equate “milder” disease classification with trivial quality-of-life burden. Studies consistently show that patients with ulcerative proctitis report significant psychological distress, social limitation, and work impairment — even when their physical disease activity scores appear low.
Tenesmus in particular — the unrelenting feeling of urgency even when the bowel is empty — is one of the most psychologically taxing IBD symptoms. It disrupts sleep, triggers anxiety about access to bathrooms, and can cause patients to avoid social situations.
Gut Health, the Microbiome, and Managing Inflammation
Whether the diagnosis is ulcerative proctitis or pancolitis, one emerging area of clinical focus is the role of the intestinal microbiome in disease activity. Both conditions are associated with dysbiosis — an imbalance in the gut bacterial ecosystem — that can perpetuate inflammation and reduce the efficacy of medical therapy.
Patients with UC show consistent depletion of short-chain fatty acid-producing bacteria (such as Faecalibacterium prausnitzii and Roseburia species) that normally protect the colonic mucosa. Restoring microbial balance through diet and carefully selected supplementation is an active area of research.
Probiotics are not a treatment for UC, but some strains have shown modest benefit in supporting remission maintenance — particularly VSL#3 and E. coli Nissle 1917 in clinical trials. If you’re considering probiotic supplementation alongside your IBD treatment, our guide on probiotic side effects explains what to watch for and how to introduce supplementation safely.
For those whose IBD overlaps with irritable bowel syndrome symptoms — which is more common than many realize — our evidence-based review of the best probiotics for IBS identifies which strains have the most clinical support for symptom relief without aggravating inflammation.
Bloating and abdominal discomfort during remission are frequent complaints that go underreported in IBD clinic visits. If these are part of your experience, our guide to the best probiotics for bloating covers targeted options with real evidence behind them.
Understanding the broader gut health landscape — including how prebiotics and probiotics differ in function — can help you have more productive conversations with your gastroenterologist. Our comparison of probiotics vs prebiotics is a solid starting point.
Practical Advice for Living With Ulcerative Proctitis or UC
Getting the Most From Your Medical Appointments
- Track your symptoms daily. A simple symptom diary — number of bowel movements, presence of blood, pain level, urgency — gives your gastroenterologist objective data that changes clinical decisions.
- Don’t skip follow-up colonoscopies. Especially for proctitis patients, surveillance is how proximal extension is caught early — before it becomes extensive colitis.
- Report tenesmus specifically. Many patients don’t mention urgency and rectal pressure because they assume it’s “just part of the condition.” It isn’t untreatable — and reporting it accurately leads to better-targeted therapy.
- Ask about treat-to-target. Modern IBD management aims for mucosal healing — not just symptom control. Ask your doctor whether endoscopic remission is being used as a goal in your care plan.
Diet and Lifestyle During Flares and Remission
- Low-residue diet during active symptoms: White rice, cooked vegetables, lean protein, and avoiding raw high-fiber foods reduces stool frequency and rectal irritation during flares.
- Mediterranean diet in remission: Growing evidence supports a Mediterranean-style diet (rich in olive oil, vegetables, legumes, and oily fish) for maintaining remission and reducing systemic inflammation in IBD.
- Avoid NSAIDs: Ibuprofen and aspirin are associated with IBD flares — use acetaminophen (paracetamol) for pain relief instead.
- Limit alcohol: Alcohol disrupts gut permeability and is a documented trigger for UC flares, particularly beer (due to sulfites and fermented components).
- Manage stress actively: The gut-brain axis creates a bidirectional relationship between psychological stress and intestinal inflammation. CBT, mindfulness-based stress reduction, and regular aerobic exercise all have evidence supporting their role in IBD symptom management.
For authoritative clinical guidance on both conditions, the Crohn’s & Colitis Foundation provides comprehensive, regularly updated patient resources. For clinicians, the European Crohn’s and Colitis Organisation (ECCO) Clinical Guidelines set the international standard for UC diagnosis and treatment protocols, including specific recommendations for ulcerative proctitis management.
Frequently Asked Questions
Conclusion: Understanding the Difference Changes Your Outcome
The distinction between ulcerative colitis vs ulcerative proctitis is not just a technicality on a pathology report. It defines which treatments you need, which risks you carry long-term, how frequently you need monitoring, and what “doing well” actually looks like for your specific disease.
Ulcerative proctitis is the most manageable form of ulcerative colitis — but manageable doesn’t mean trivial. Symptoms can be deeply disruptive. And without proper treatment achieving mucosal healing, the risk of the disease extending further into the colon is real and meaningful.
Whether you have proctitis or more extensive UC, the most important step is working with a gastroenterologist who treats to the goal of complete mucosal remission — not just absence of symptoms. Know your disease extent. Understand your treatment rationale. Keep your surveillance appointments. And don’t minimize symptoms that affect your daily life just because you’ve been told your disease is “mild.”
This article is for informational and educational purposes only and does not constitute medical advice. Always consult a licensed gastroenterologist regarding your individual diagnosis and treatment plan. See our full medical disclaimer.